

In December 2025, orthopedic care at St. Joseph’s Health in Syracuse entered a new, exciting chapter: a brand-new practice, St. Joseph’s Health Orthopedic and Spine Care, was launched as part of St. Joseph’s Physicians. With offices located in Fayetteville and Camillus, the practice includes a team of five board-certified, fellowship-trained surgeons: Kevin Kopko, MD, Medical Director of Joint Surgery; Bradley Raphael, MD, Medical Director of Sports Medicine; Aaron Bianco, MD; Justin Iorio, MD, Medical Director of Spine Surgery; and Prashant Deshmane, MD.
 Although the practice is new, the providers each bring over ten years of experience gained by
Although the practice is new, the providers each bring over ten years of experience gained by
practicing orthopedics and spine care both locally and around the country. “Early on,
when you start right out of fellowship, experience can be lacking. But with us in this practice,
all of us have a combined 50-plus years of experience. To me, that’s a huge differentiating point that distinguishes us from other practices,” said Dr. Deshmane, who specializes in adult
reconstruction, shoulder surgery and sports medicine, and is the most recent addition to the team of surgeons, joining the practice in April.
In addition to depth of experience, each provider brings sub-specialty orthopedic expertise, from joint replacement to spine surgery, sports medicine, and neck and back care, that all add up to a largely comprehensive service line offering that’s highly accessible to both referring providers and patients, alike.
“I think that we have a really knowledgeable, comprehensive team that offers great access
to high-quality care,” said Dr. Iorio.
Sub-Specialty Depth in an Integrated Setting
 As the single orthopedic and spine practice integrated within the hospital system, St. Joseph’s Health Orthopedic and Spine Care can quickly connect with many specialized health care providers, offering the “best of both worlds” from inpatient and outpatient care, as Dr. Raphael explained.
As the single orthopedic and spine practice integrated within the hospital system, St. Joseph’s Health Orthopedic and Spine Care can quickly connect with many specialized health care providers, offering the “best of both worlds” from inpatient and outpatient care, as Dr. Raphael explained.
“I think something that sets us apart from other practices is that interdisciplinary ability and service that we can provide for patients by having multi-specialties – not just multi-orthopedic specialties, but multi-medical specialties, as well,” Dr. Raphael said. If the surgeons have a question for or need to set up an appointment with other practitioners, such as cardiologists or neurologists, those connections are just a phone call or message away. “I have all these resources at my disposal, literally at my fingertips through our electronic medical records system, EPIC. On top of that, it’s an outpatient office. It’s really a great interdisciplinary program.”
 Dr. Raphael, who was born and raised in Syracuse, followed in the footsteps of his father, Dr.
Dr. Raphael, who was born and raised in Syracuse, followed in the footsteps of his father, Dr.
Irving Raphael, to practice sports medicine. He also specializes in shoulder and knee treatment, as well as cartilage and joint preservation. Both he and Dr. Deshmane have provided care for professional athletes and major sports teams around the country.
When it comes to joint surgery, Dr. Kopko specializes in both full hip and knee replacement, as well as partial knee replacement and revision surgery for previous joint replacements. He emphasized that the practice sees many patients who are looking for a second opinion. “We’re willing to see patients for almost anything,” said Dr. Kopko. “We’re not going to turn patients away because they’ve been seen by another orthopedic practice or had surgery elsewhere.”
The spine side of the practice is  led by Dr. Iorio, who specializes in cervical, thoracic and
led by Dr. Iorio, who specializes in cervical, thoracic and
lumbar surgery, spinal tumors and degenerative conditions, and Dr. Bianco, who specializes in treatment of the neck and back. Both Dr. Iorio and Dr. Bianco discussed the upcoming exciting addition of the EOS full-body x-ray imaging system, which will facilitate comprehensive care for patients and enhance how the group’s providers can work together across sub-specialties, as Dr. Iorio explained.
“The EOS is hugely important between spine providers and hip providers like Dr. Kopko and Dr. Deshmane because the imaging Dr. Bianco and I are getting now includes the joints they’re evaluating,” Dr. Iorio said. “I’ll see patients understanding they have a spine condition, and
learn they also have a problem in the hip joint, for example. We’re getting a better analysis of
patients and working together as a single team of orthopedic surgeons at the same time.”
Advanced Technology and Minimally Invasive Options
 The EOS is a prime example of how the St. Joseph’s Health Orthopedics and Spine Care team is utilizing the latest technology available to provide patient-centered care. Rather than stitching together separate x-ray images to get a full-picture view of patients’ needs, as was done previously, the EOS system provides 2D and 3D images of the full skeletal system, helping better inform surgeons in the planning and diagnosis process. St. Joseph’s Health Orthopedics and Spine Care is currently the only practice between Rochester and New York City to utilize this technology.
The EOS is a prime example of how the St. Joseph’s Health Orthopedics and Spine Care team is utilizing the latest technology available to provide patient-centered care. Rather than stitching together separate x-ray images to get a full-picture view of patients’ needs, as was done previously, the EOS system provides 2D and 3D images of the full skeletal system, helping better inform surgeons in the planning and diagnosis process. St. Joseph’s Health Orthopedics and Spine Care is currently the only practice between Rochester and New York City to utilize this technology.
“The EOS system can also incorporate spinal pelvic parameters, and it uses AI technology and the cloud to help inform decisions about surgical corrections, degenerative changes and spinal deformities,” Dr. Bianco explained.
 Perhaps the most well-known cutting-edge technology utilized by the new practice is one surgeons at St. Joseph’s Health Hospital have been using for many years: minimally-invasive, robotic-assisted surgery and navigation. Dr. Deshmane explained how robotics help minimize patient dissatisfaction from imprecise placement of joint replacement components, especially for younger, high-demand patients.
Perhaps the most well-known cutting-edge technology utilized by the new practice is one surgeons at St. Joseph’s Health Hospital have been using for many years: minimally-invasive, robotic-assisted surgery and navigation. Dr. Deshmane explained how robotics help minimize patient dissatisfaction from imprecise placement of joint replacement components, especially for younger, high-demand patients.
“For these patients, it’s important to make sure you do the joint replacement surgery in a way that’s personalized, meaning your shoulder is different than my shoulder, is different than somebody else’s shoulder,” stated Dr. Deshmane. “Whether it’s computer navigation or robotics, these advanced technologies allow us to dial in on placement of components based on each particular patient’s anatomy. That’s the reason I’m particularly interested in these technologies.”
St. Joseph’s Health also uses the TrackX surgical navigation system and is currently the only
facility in the Syracuse area to have a Mako 4 robot, which is made by Stryker. Dr. Kopko described this robot as the gold standard in robotics for joint replacement, helping to improve patient alignment and reducing risk.
“With patients who have abnormal anatomy and present a potentially challenging surgery, the
robot is kind of like a GPS guidance system to make sure you know where you’re going. It’s almost like having a second surgeon in the room because it helps you better understand and plan what to do next,” said Dr. Kopko, adding that the Mako 4 is indicated for especially complex revision surgeries on patients who’ve had a previous joint
replacement – cases which sometimes needed to be referred out in the past, but that can now be performed by the St. Joseph’s Health Orthopedic and Spine Care group.
 In the realm of sports medicine, an exciting non-surgical treatment option the practice offers is orthobiologics utilizing platelet-rich plasma, or PRP. Dr. Raphael described the treatment as a straightforward, in-office procedure that isolates platelets, or growth factors, from the patient’s blood, and then injects them in the needed areas, healing the body with its own tissue rather than a foreign substance that may cause additional tissue deterioration. He said it’s especially useful for treating early arthritis, helping to regrow deteriorated cartilage in a less invasive way. Orthobiologics is one way the team is working on injury prevention and surgery avoidance in sports medicine, Dr. Raphael emphasized.
In the realm of sports medicine, an exciting non-surgical treatment option the practice offers is orthobiologics utilizing platelet-rich plasma, or PRP. Dr. Raphael described the treatment as a straightforward, in-office procedure that isolates platelets, or growth factors, from the patient’s blood, and then injects them in the needed areas, healing the body with its own tissue rather than a foreign substance that may cause additional tissue deterioration. He said it’s especially useful for treating early arthritis, helping to regrow deteriorated cartilage in a less invasive way. Orthobiologics is one way the team is working on injury prevention and surgery avoidance in sports medicine, Dr. Raphael emphasized.
“Many injuries can be prevented, and we’re trying to educate patients and use non-operative, less invasive treatments with physical therapy as much as possible,” said Dr. Raphael. Dr. Bianco echoed this strategy, explaining that treatment decisions are patient-centered and aimed at the most conservative, least invasive methods available: “Our goal is focused on patient outcomes. We want excellent patient outcomes, patient satisfaction, and improved patient function.”
Efficient Access, Communication and Continuity of Care
 An important aspect of the new practice that greatly enhances patient experience is improved access for both patients and referring providers alike, made possible by the group’s integration within the St. Joseph’s Health network. Rather than communicating via text messages or phone calls as they did before, St. Joseph’s Health practitioners now use Epic, one of the biggest medical record systems in the world, to send messages instantly to each other directly within patients’ charts. This improvement in communication
An important aspect of the new practice that greatly enhances patient experience is improved access for both patients and referring providers alike, made possible by the group’s integration within the St. Joseph’s Health network. Rather than communicating via text messages or phone calls as they did before, St. Joseph’s Health practitioners now use Epic, one of the biggest medical record systems in the world, to send messages instantly to each other directly within patients’ charts. This improvement in communication
allows more care coordination between referring physicians and surgeons, including consult feedback, co-management of patient needs and post-procedure follow-up.
“It’s infinitely easier when you’re on one medical record system to talk to primary care doctors and to follow patients. Patients can also message us directly through MyChart, which is huge, and they can make appointments through that system as well. It’s the standard across many healthcare facilities in our area – not just at St. Joseph’s,” stated Dr. Kopko.
Whether patients come into the practice through referrals from their primary care providers or if they contact the practice directly for an appointment – which is more common with younger patients needing sports medicine treatments in particular – each member of the practice emphasized how patients can be seen quickly. This ease of access helps overcome traditional barriers to care.
“I think that above all else, we want providers to be able to refer to us so we can get patients seen and there aren’t any barriers. We really try to make it easy for them, and we welcome them to reach out to us directly,” said Dr. Iorio. Both clinic locations offer walk-in hours, and most patients can be seen within a week, if not on the same day. Dr. Iorio also explained that patients are seen on a timely schedule following surgery or treatments, often for at least one or two years.
More Growth to Come in Years Ahead
 Reflecting on the success of the practice so far and looking ahead to what’s next, the surgeons at St. Joseph’s Health Orthopedics and Spine Care are excited to build on the team’s progress and momentum.
Reflecting on the success of the practice so far and looking ahead to what’s next, the surgeons at St. Joseph’s Health Orthopedics and Spine Care are excited to build on the team’s progress and momentum.
“I’ve been practicing at St. Joseph’s for 15 years now, so for me, I knew how great of a place it is,” said Dr. Raphael. “I knew how incredible of a hospital system it is, with all the ancillary and inter disciplinary services. I knew that St. Joseph’s had all these incredible programs for a long time, but it didn’t have a dedicated orthopedics department. This has been a great opportunity to help build this department within the St. Joseph’s network.”
“I think for myself and my partners, we’re extremely happy with our new roles within St. Joseph’s and how the practice has treated us and allowed us to grow even in just the first four months. We’re very blessed to be part of this new practice,” said Dr. Bianco. “There’s an intent to expand the practice to essentially all orthopedic sub-specialties, like hand, foot and ankle, and ultimately a third location, which will allow us to bring on more providers as space allows.”
It all comes down to providing the highest level of care to patients, however, as Dr. Deshmane emphasized. “Looking at it from a patient’s perspective, they just want to know that they have options,” he said. “Our practice comes up as a very valid option in our community, with a lot of experience under our belt.”
the highest level of care to patients, however, as Dr. Deshmane emphasized. “Looking at it from a patient’s perspective, they just want to know that they have options,” he said. “Our practice comes up as a very valid option in our community, with a lot of experience under our belt.”

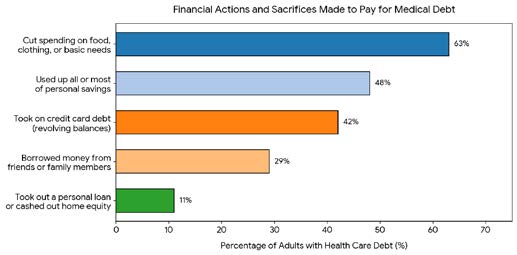 Interesting conversation with a patient last week about their mounting health care debt. Higher premiums, higher deductibles, higher co-pays, more out of formulary uncovered meds all adding up to $45,000 in annual out of pocket costs.
Interesting conversation with a patient last week about their mounting health care debt. Higher premiums, higher deductibles, higher co-pays, more out of formulary uncovered meds all adding up to $45,000 in annual out of pocket costs.
 Disputes in the health care sector are inevitable. Whether they arise between physicians in a group practice, between an ambulatory surgical center and its member surgeons, or between a hospital system and an affiliated provider, conflicts over governance, compensation, non-compete agreements, or operational decisions can quickly consume the time, energy, and resources of all involved. Litigation has long been the default mechanism for resolving such conflicts, but it is rarely the best one. Mediation particularly when guided by an experienced health care attorney serving as mediator offers a faster, more cost effective, and more relationship-preserving alternative that deserves serious consideration.
Disputes in the health care sector are inevitable. Whether they arise between physicians in a group practice, between an ambulatory surgical center and its member surgeons, or between a hospital system and an affiliated provider, conflicts over governance, compensation, non-compete agreements, or operational decisions can quickly consume the time, energy, and resources of all involved. Litigation has long been the default mechanism for resolving such conflicts, but it is rarely the best one. Mediation particularly when guided by an experienced health care attorney serving as mediator offers a faster, more cost effective, and more relationship-preserving alternative that deserves serious consideration.
 Berlucchi had previously worked for Lancaster General Hospital in Lancaster, Pennsylvania and had come to understand how important OBGYN care is for women in rural and underserved populations. “I know what it’s like to be geographically separated from a maternity center,” he explained. Berlucchi partnered with Crouse Hospital to maintain obstetrical services at Auburn Community Hospital.
Berlucchi had previously worked for Lancaster General Hospital in Lancaster, Pennsylvania and had come to understand how important OBGYN care is for women in rural and underserved populations. “I know what it’s like to be geographically separated from a maternity center,” he explained. Berlucchi partnered with Crouse Hospital to maintain obstetrical services at Auburn Community Hospital. ACH as Chief of Obstetrics and Gynecology. A primary reason she decided to join ACH is the small-town community feeling where she can grow meaningful relationships with patients.
ACH as Chief of Obstetrics and Gynecology. A primary reason she decided to join ACH is the small-town community feeling where she can grow meaningful relationships with patients. Dr. Bonilla-Martir explained that she also felt drawn to ACH because the obstetrics and gynecology programs are integrated, and that while some complicated cases may need to be referred out to providers in Rochester or Syracuse, they are able to take on many high-risk patients as well as normal pregnancies.
Dr. Bonilla-Martir explained that she also felt drawn to ACH because the obstetrics and gynecology programs are integrated, and that while some complicated cases may need to be referred out to providers in Rochester or Syracuse, they are able to take on many high-risk patients as well as normal pregnancies.  “Many patients love Dr. Balaya,” said Dr. Bonilla Martir. “As of the beginning of April, he has become a full time physician with us and will be helping us continue to deliver the high-quality care that women in the community need.”
“Many patients love Dr. Balaya,” said Dr. Bonilla Martir. “As of the beginning of April, he has become a full time physician with us and will be helping us continue to deliver the high-quality care that women in the community need.” Another stand-out aspect of the team of OBGYN providers at ACH is the personalized care provided by the staff of midwives. Jennifer MacBlane, CNM, had been coming to ACH on and off for several years before joining the team full time in August of 2025. She echoed the sentiments of her colleagues when it comes to the small community feel of ACH and of the wider Auburn community.
Another stand-out aspect of the team of OBGYN providers at ACH is the personalized care provided by the staff of midwives. Jennifer MacBlane, CNM, had been coming to ACH on and off for several years before joining the team full time in August of 2025. She echoed the sentiments of her colleagues when it comes to the small community feel of ACH and of the wider Auburn community. “The word ‘midwife’ means ‘with woman.’ The whole idea is that we’re with them to help them and develop whatever they need,” MacBlane said. “It’s all-encompassing. Midwives kind of look at the big picture, so we include everybody – your family, your social history, your medical history. We put it all together. It’s a really nice, unique experience because you get a little bit of the warm and fuzzy, but we also do the medical side. We can get you medicine, lab work, testing, we can get you an epidural – we’re qualified to do that. We just look at it a little differently, and we work a little closer with the patient while they’re in labor.”
“The word ‘midwife’ means ‘with woman.’ The whole idea is that we’re with them to help them and develop whatever they need,” MacBlane said. “It’s all-encompassing. Midwives kind of look at the big picture, so we include everybody – your family, your social history, your medical history. We put it all together. It’s a really nice, unique experience because you get a little bit of the warm and fuzzy, but we also do the medical side. We can get you medicine, lab work, testing, we can get you an epidural – we’re qualified to do that. We just look at it a little differently, and we work a little closer with the patient while they’re in labor.” “We work together as a group,” shared MacBlane. “Midwives are independent in New York State, but we work together with the physicians to kind of cover our patients and determine the plan for their care collaboratively, which is really nice.”
“We work together as a group,” shared MacBlane. “Midwives are independent in New York State, but we work together with the physicians to kind of cover our patients and determine the plan for their care collaboratively, which is really nice.” recent years and now includes a dedicated women’s imaging center within the hospital. Jubin Jacob, MD, Chair of Radiology at ACH, highlighted advancements in mammography technology offered to women at ACH, including stereotactic biopsies utilizing mammographic guidance and ultrasound equipment that provides 3D images while keeping radiation doses as low as possible. He emphasized how all the technological advancements offered to women at ACH are aimed at enhancing patient experience.
recent years and now includes a dedicated women’s imaging center within the hospital. Jubin Jacob, MD, Chair of Radiology at ACH, highlighted advancements in mammography technology offered to women at ACH, including stereotactic biopsies utilizing mammographic guidance and ultrasound equipment that provides 3D images while keeping radiation doses as low as possible. He emphasized how all the technological advancements offered to women at ACH are aimed at enhancing patient experience. With the opening of the new Interventional Radiology suite and the recent addition of a physician assistant who will primarily work on further expansion of radiology services, Dr. Jacob said several other advanced treatments and procedures are being offered to women at ACH. Examples of these new offerings are minimally invasive procedures to treat symptomatic fibroids, adenomyosis, and pelvic venous insufficiency, as well as curative ablation treatments for breast cancer tumors in patients who are not surgical candidates. In addition, the team has access to the best quality PET scanner in the region.
With the opening of the new Interventional Radiology suite and the recent addition of a physician assistant who will primarily work on further expansion of radiology services, Dr. Jacob said several other advanced treatments and procedures are being offered to women at ACH. Examples of these new offerings are minimally invasive procedures to treat symptomatic fibroids, adenomyosis, and pelvic venous insufficiency, as well as curative ablation treatments for breast cancer tumors in patients who are not surgical candidates. In addition, the team has access to the best quality PET scanner in the region. With anticipated changes to the demographics of people in areas surrounding ACH – including a population that’s both aging and also growing due to developments like Micron – Berlucchi is passionate about continuing to expand the OBGYN practice at the health center. Currently in the process of obtaining a grant with the Department of Health, Berlucchi is leading the team toward a vision of comprehensive healthcare for women of all ages including OBGYN and beyond.
With anticipated changes to the demographics of people in areas surrounding ACH – including a population that’s both aging and also growing due to developments like Micron – Berlucchi is passionate about continuing to expand the OBGYN practice at the health center. Currently in the process of obtaining a grant with the Department of Health, Berlucchi is leading the team toward a vision of comprehensive healthcare for women of all ages including OBGYN and beyond.
 I am an avid reader, belong to two book clubs, and receive a steady stream of great recommendations from my health news feed. Recently, I had the opportunity to read two excellent books by local physician authors: Dr. Mary Jumbelic, retired Chief Medical Examiner of Onondaga County, and Dr. Sarah Matt, surgeon and health technology expert. Two very different books, but both outstanding and musts for your reading list.
I am an avid reader, belong to two book clubs, and receive a steady stream of great recommendations from my health news feed. Recently, I had the opportunity to read two excellent books by local physician authors: Dr. Mary Jumbelic, retired Chief Medical Examiner of Onondaga County, and Dr. Sarah Matt, surgeon and health technology expert. Two very different books, but both outstanding and musts for your reading list. I asked Dr. Jumbelic when she first realized she wanted to write. Throughout her career, she kept journals and notes about her work, not realizing how important they would be later in life. After retiring, she entered a writing contest and then began taking classes, evolving into a seasoned author with an incredible voice that merges technical forensic expertise with deeply personal reflection.
I asked Dr. Jumbelic when she first realized she wanted to write. Throughout her career, she kept journals and notes about her work, not realizing how important they would be later in life. After retiring, she entered a writing contest and then began taking classes, evolving into a seasoned author with an incredible voice that merges technical forensic expertise with deeply personal reflection. Dr. Sarah Matt has also drawn on her surgical and technical expertise to write a strategic and highly readable look at the future of technology in health care. A mid-career physician, she has broadened her impact by working across the health technology landscape, including leadership roles with health technology companies and digital health initiatives.
Dr. Sarah Matt has also drawn on her surgical and technical expertise to write a strategic and highly readable look at the future of technology in health care. A mid-career physician, she has broadened her impact by working across the health technology landscape, including leadership roles with health technology companies and digital health initiatives.

 To safeguard patient care from corporate interference in clinical decisionmaking, New York maintains one of the strictest corporate practice of medicine (“CPOM”) prohibitions in the United States. Under New York law, medical services may be provided only by licensed medical professionals, by professional entities that are owned and controlled exclusively by licensed medical professionals, or by hospitals and other entities expressly authorized under the Public Health Law.
To safeguard patient care from corporate interference in clinical decisionmaking, New York maintains one of the strictest corporate practice of medicine (“CPOM”) prohibitions in the United States. Under New York law, medical services may be provided only by licensed medical professionals, by professional entities that are owned and controlled exclusively by licensed medical professionals, or by hospitals and other entities expressly authorized under the Public Health Law.
 The arrival of Dr. Jorge Romero as Section Chief of Cardiac Electrophysiology and Director of Cardiovascular Research and Innovation is a prime example of increased convenience and accessibility for patients, bringing cutting edge treatments directly into their community. Dr. Taub noted that she initially connected with Dr. Romero to refer a patient for a procedure that couldn’t be done locally.
The arrival of Dr. Jorge Romero as Section Chief of Cardiac Electrophysiology and Director of Cardiovascular Research and Innovation is a prime example of increased convenience and accessibility for patients, bringing cutting edge treatments directly into their community. Dr. Taub noted that she initially connected with Dr. Romero to refer a patient for a procedure that couldn’t be done locally. “Instead of heating or freezing the tissue, we are creating small holes in the cell membrane, called electroporation. The beauty of this technology is that the cardiac muscle is uniquely sensitive. We only need a small dose of energy to eliminate the triggers for atrial fibrillation located in the pulmonary veins of the patient,” Dr. Romero said, which avoids damage to the smooth muscle of the esophagus, phrenic nerves, and other adjacent structures. This has eliminated the risk of atrial esophageal fistula, a deadly complication that used to happen in 0.2% of ablation cases, but which hasn’t occurred in the 800,000 cases of PFA that have been performed so far worldwide. This new, safer technology greatly benefits the older population, mostly over the ages of 70, who are most likely to suffer from atrial fibrillation, offering improved quality of life and reducing longterm risks. Dr. Romero successfully performed Upstate’s first ablation using the Affera Mapping and Ablation System with the Sphere-9 catheter, a multi-purpose catheter not found at any other facility in New York State outside New York city and Long Island.
“Instead of heating or freezing the tissue, we are creating small holes in the cell membrane, called electroporation. The beauty of this technology is that the cardiac muscle is uniquely sensitive. We only need a small dose of energy to eliminate the triggers for atrial fibrillation located in the pulmonary veins of the patient,” Dr. Romero said, which avoids damage to the smooth muscle of the esophagus, phrenic nerves, and other adjacent structures. This has eliminated the risk of atrial esophageal fistula, a deadly complication that used to happen in 0.2% of ablation cases, but which hasn’t occurred in the 800,000 cases of PFA that have been performed so far worldwide. This new, safer technology greatly benefits the older population, mostly over the ages of 70, who are most likely to suffer from atrial fibrillation, offering improved quality of life and reducing longterm risks. Dr. Romero successfully performed Upstate’s first ablation using the Affera Mapping and Ablation System with the Sphere-9 catheter, a multi-purpose catheter not found at any other facility in New York State outside New York city and Long Island. “It’s less morbid; recovery is fast, and outcomes are very similar to open-heart surgery,” said Dr. Kalra. “Transcatheter techniques for the aortic valve are becoming the procedure of choice. Even patients who are at low risk for complications following open heart surgery are eligible for and favor the transcatheter heart valve due to significantly less morbidity following the procedure, and faster return to normal life.”
“It’s less morbid; recovery is fast, and outcomes are very similar to open-heart surgery,” said Dr. Kalra. “Transcatheter techniques for the aortic valve are becoming the procedure of choice. Even patients who are at low risk for complications following open heart surgery are eligible for and favor the transcatheter heart valve due to significantly less morbidity following the procedure, and faster return to normal life.” Foundational to cardiovascular care is cardiovascular imaging, which is used not only for visualizing and diagnosing cardiac disease, but also during interventional procedures. Under the guidance of Dr. Adeeb Al-Quthami, Director of Cardiovascular Imaging, significant investments in the latest technology have been secured for the benefit of Upstate’s patients.
Foundational to cardiovascular care is cardiovascular imaging, which is used not only for visualizing and diagnosing cardiac disease, but also during interventional procedures. Under the guidance of Dr. Adeeb Al-Quthami, Director of Cardiovascular Imaging, significant investments in the latest technology have been secured for the benefit of Upstate’s patients. “We can visualize the heart to a very high degree in terms of tiny detail,” he said. “If you try to take a picture of something that’s moving, it’s going to blur, especially if what you’re trying to take a picture of is small. With the advancements in technology, we can take a picture of the heart within a fraction of a heartbeat,” identifying patients’ unique anatomy and offering precise, personalized treatment for each patient.
“We can visualize the heart to a very high degree in terms of tiny detail,” he said. “If you try to take a picture of something that’s moving, it’s going to blur, especially if what you’re trying to take a picture of is small. With the advancements in technology, we can take a picture of the heart within a fraction of a heartbeat,” identifying patients’ unique anatomy and offering precise, personalized treatment for each patient. Launched within the last year, AI assisted plaque analysis software, called HeartFlow, is now helping the Upstate cardiovascular team to better assess a patient’s risk for a future heart attack. Dr. Al-Quthami explained how this new technology offers improvement over the traditional coronary calcium scan.
Launched within the last year, AI assisted plaque analysis software, called HeartFlow, is now helping the Upstate cardiovascular team to better assess a patient’s risk for a future heart attack. Dr. Al-Quthami explained how this new technology offers improvement over the traditional coronary calcium scan. By recruiting more cardiovascular experts to Upstate and continuing to invest in the innovative technologies they use, Dr. Tucker highlighted how the Upstate cardiovascular program is committed to staying at the forefront of cardiovascular care.
By recruiting more cardiovascular experts to Upstate and continuing to invest in the innovative technologies they use, Dr. Tucker highlighted how the Upstate cardiovascular program is committed to staying at the forefront of cardiovascular care.
 When Melanie McNally, MD first began practicing urology, she didn’t anticipate developing a focus on urologic issues specific to women. However, about five years into her practice, she found many women were experiencing urologic health concerns that gynecology was illequipped to manage.
When Melanie McNally, MD first began practicing urology, she didn’t anticipate developing a focus on urologic issues specific to women. However, about five years into her practice, she found many women were experiencing urologic health concerns that gynecology was illequipped to manage. Stallone has held two unwavering truths: he wanted to be a physician, and he wanted to serve his country. Both were anchored by clear purpose.
Stallone has held two unwavering truths: he wanted to be a physician, and he wanted to serve his country. Both were anchored by clear purpose. He went on to earn both an MD and MBA simultaneously from the University of Pennsylvania, and later an MA in National Security Policy Studies from the U.S. Naval War College. He also serves as an Air Force Colonel and has been with the New York Air National Guard for more than 28 years, the past seven as the New York State Air Surgeon. These accomplishments reflect a career built on discipline, leadership, and a breadth of perspective informed by medicine, business, and service.
He went on to earn both an MD and MBA simultaneously from the University of Pennsylvania, and later an MA in National Security Policy Studies from the U.S. Naval War College. He also serves as an Air Force Colonel and has been with the New York Air National Guard for more than 28 years, the past seven as the New York State Air Surgeon. These accomplishments reflect a career built on discipline, leadership, and a breadth of perspective informed by medicine, business, and service. As his career evolved, Dr. Stallone stepped into health system leadership roles, including serving as a hospitalist, physician leader, and former health system CEO, gaining a broader view of how care is delivered and where it often breaks down. He saw firsthand the pressures facing providers, the operational realities behind clinical decisions, and the importance of aligning strategy with real world practice.
As his career evolved, Dr. Stallone stepped into health system leadership roles, including serving as a hospitalist, physician leader, and former health system CEO, gaining a broader view of how care is delivered and where it often breaks down. He saw firsthand the pressures facing providers, the operational realities behind clinical decisions, and the importance of aligning strategy with real world practice. That belief drew him to Excellus BlueCross BlueShield (Excellus BCBS) well before his executive appointment. Through his involvement on the plan’s Central New York and Southern Tier regional advisory boards and governing board of directors, Dr. Stallone developed a deeper understanding of the organization’s nonprofit mission and its commitment to community-focused care. Just as important, he learned the value of listening. “You have to understand providers, the community, payors, and the people doing the work,” he says. “That’s how you design programs that actually make a difference.”
That belief drew him to Excellus BlueCross BlueShield (Excellus BCBS) well before his executive appointment. Through his involvement on the plan’s Central New York and Southern Tier regional advisory boards and governing board of directors, Dr. Stallone developed a deeper understanding of the organization’s nonprofit mission and its commitment to community-focused care. Just as important, he learned the value of listening. “You have to understand providers, the community, payors, and the people doing the work,” he says. “That’s how you design programs that actually make a difference.” At the core of his vision is partnership. Drawing on his experience as both a physician and a former health system CEO, Dr. Stallone sees collaboration as the most effective path forward in an increasingly complex healthcare environment. He designs practical, sustainable, and impactful programs by grounding his strategy in the real challenges facing the healthcare system, including rising costs.
At the core of his vision is partnership. Drawing on his experience as both a physician and a former health system CEO, Dr. Stallone sees collaboration as the most effective path forward in an increasingly complex healthcare environment. He designs practical, sustainable, and impactful programs by grounding his strategy in the real challenges facing the healthcare system, including rising costs.  Dr. Stallone envisions Excellus BCBS as a bridge-builder, bringing together providers, health systems, and community partners to solve problems collaboratively. His focus is on creating pathways that strengthen relationships, improve coordination, and deliver measurable improvements in care—all while staying true to the organization’s mission.
Dr. Stallone envisions Excellus BCBS as a bridge-builder, bringing together providers, health systems, and community partners to solve problems collaboratively. His focus is on creating pathways that strengthen relationships, improve coordination, and deliver measurable improvements in care—all while staying true to the organization’s mission.