



Maya Mathew, MD, Medical Director of Radiation Oncology

Patients benefit from on-site simulation CT and advanced imaging located conveniently on campus. Rossi is pictured.
Peer-Review by Disease-Site Specialists
Once a treatment plan has been designed by Dr. Mathew, it is presented at a peer-review conference where all the Roswell park radiation oncologists examine the treatment plan. This process is adhered to for every patient. The peer-review board has disease-site specialists who perform a rigorous review of every proposed treatment plan across Roswell Park’s outpatient network. The board dissects the plans, ensures that all dose limits are met, field arrangements are optimal, comorbidities are properly considered and makes any suggestions for improvement.
“The board is made up of different radiation oncologists who treat specific disease sites, so I’m getting the expertise from specialized physicians who are reviewing my treatment plans,” Dr. Mathew says. “That is an assurance for the patient and the referring providers that they are getting the best possible care.”
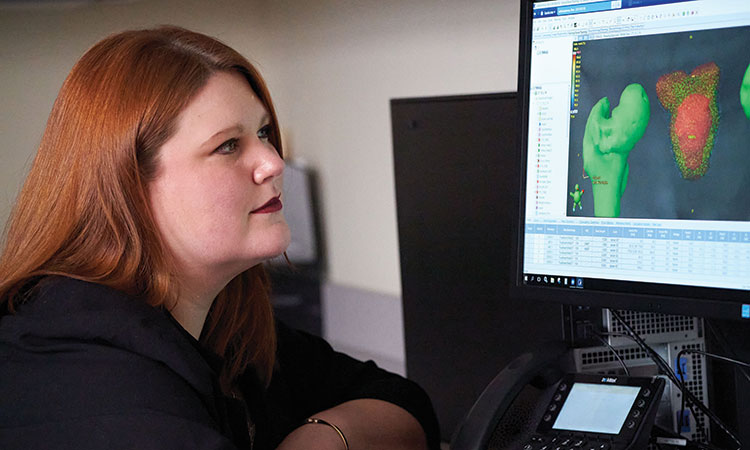
During the treatment planning phase, Dr. Mathew and Roswell Park Dosimetrist, Vanessa Rundle, MS, CMD, RT(R)(T), conduct anatomical contouring using CT images, which is both an art and a science to advanced treatment planning.
Quality Assurance for Every Patient
Once the peer-review board has ensured a plan meets Roswell Park safety protocols and provides the best approach to treatment, an onsite Roswell physicist performs end-to-end quality assurance tests. The quality assurance conducted by the physicist validates the treatment plan will be delivered as prescribed. If any part of the plan does not meet Roswell standards, treatment will not be administered and the plan will be reevaluated. This process is performed for every patient receiving care at the center.
“The quality assurance piece with the help of our physics team is essential. They have their protocols to follow and if the plan does not adhere to Roswell standards, the plan will not be approved to roll out,” Dr. Mathew says. “It is a long process but in the end the patient can be assured that they receive the best care.”
In addition to internal quality assurance, the center also participates in third party review to further validate the quality of treatment plans being delivered. The review is completed by the MD Anderson Imaging and Radiation Oncology Core (IROC) Quality Assurance Center in Houston, Texas.

The center is equipped with TrueBeam radiotherapy, the most advanced linear accelerator and radiosurgery treatment system available. Pictured from left to right: Meghann Wright, RT(T), and Rossi
Excellence in Treatment Delivery
At Oneida Health, the quality of cancer treatment delivery is a combination of state-of-the-art technology and staff expertise. Radiation therapists use a TrueBeam linear accelerator to generate and deliver precise photon beams to tumors in the body, as well as Stereotactic Beam Radiation Therapy (SBRT) to deliver a course of therapy in a condensed timeframe. Radiation therapists also employ motion management (RGSC- Respiratory Gating for Scanners), DIBH (Deep inspiration breath hold), and prone breast radiation therapy techniques to reduce unnecessary radiation doses to healthy organs.
“We have cutting edge treatment systems here in the building so the patient does not have to go anywhere else. But the expertise of the staff, in the field of cancer care, is the difference,” Dr. Mathew says.
Oneida Health staff are also trained to educate the patient about what treatment they are getting and why, making the patient a partner in the treatment they receive and providing them with comfort along the way.
“Each cancer patient is close to my heart,” Dr. Mathew says. “Walking them through their treatments to completion, and achieving the best patient outcome; that is most rewarding for me. The patient experience is an essential ingredient to the delivery of a quality treatment plan.”

Collaboration of a highly skilled team of employees is the difference in providing and meeting stringent quality treatment measures at the center. Pictured left to right: Kare Nicholas, RN, BSN, and Chief Radiation Therapist/Radiation Oncology Center Manager Shaun Maroney, RT(T), MHA
Cohesive Patient Care
Patients and providers who choose Oneida Health will also benefit from the collaboration and continuum of care between medical oncology, radiation oncology and the imaging centers on campus. The William L. Griffin Medical Oncology Center, which opened in 2017, offers 12 infusion suites, a hematology/oncology outpatient office and is directed by a Roswell Park-affiliated physician who provides evaluations, chemotherapy infusions, palliative medicine, hematology, nutrition services, and several cancer screening services. As part of a three phase plan to oncology, Oneida Health has also invested in the expansion of their imaging, which now includes a 3 Tesla MRI, CT Simulation, PET/CT, nuclear medicine camera and a second 3D mammography machine.
“This cohesive, high-quality cancer care program was the singular vision of the Roswell Park and Oneida Health partnership from the start,” Morreale says. “Because of valued relationships with the Griffins and Gormans, as well as Roswell Park, we can now provide the very best cancer care to Central New Yorkers right in Oneida.”
For more information about Radiation Oncology at Oneida Health, visit oneidacancer.org.




 “There has always been support 100% of the time for every emergency case, and it’s a huge responsibility for us to be able to provide the kind of care we provide to the community. It is a privileged role we have, and I feel fortunate that we are fully supported to take care of our patients and make sure they get the best treatment possible.”
“There has always been support 100% of the time for every emergency case, and it’s a huge responsibility for us to be able to provide the kind of care we provide to the community. It is a privileged role we have, and I feel fortunate that we are fully supported to take care of our patients and make sure they get the best treatment possible.”













 Matthew Chaffin, MD, Compliance Officer
Matthew Chaffin, MD, Compliance Officer



 Bluetooth stethoscope
Bluetooth stethoscope




 Ruham Nasany, MD, is leading a multi-disciplinary team for the new Neuro-Oncology program.
Ruham Nasany, MD, is leading a multi-disciplinary team for the new Neuro-Oncology program.
 Satish Krishnamurthy, MD, leads the Neurosurgery department and is a funded researcher. In Fall 2020 he received a $324,000 DOD grant to find a pharmacological solution for hydrocephalus instead of repeated shunt surgery.
Satish Krishnamurthy, MD, leads the Neurosurgery department and is a funded researcher. In Fall 2020 he received a $324,000 DOD grant to find a pharmacological solution for hydrocephalus instead of repeated shunt surgery.
 Robert Beach, MD, monitoring patient Amyee Rodriguez of Gouverneur, New York
Robert Beach, MD, monitoring patient Amyee Rodriguez of Gouverneur, New York Frozen samples of brain cancer tumors can be carefully thawed, put in a nourishing medium and placed in a body-temperature incubator to bring them back to life at Upstate’s Brain Tumor Research Laboratory.
Frozen samples of brain cancer tumors can be carefully thawed, put in a nourishing medium and placed in a body-temperature incubator to bring them back to life at Upstate’s Brain Tumor Research Laboratory.



 Dr. Wickline (center) with Uday Myneni, MS, MBBS, MCH, and his resident team at the first annual arthroplasty conference in Hyderabad, India. Dr. Wickline performed the first anterior hip replacement with the HANA table, televised live to over 400 surgeons.
Dr. Wickline (center) with Uday Myneni, MS, MBBS, MCH, and his resident team at the first annual arthroplasty conference in Hyderabad, India. Dr. Wickline performed the first anterior hip replacement with the HANA table, televised live to over 400 surgeons.